AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2642-9756/023
1 Department of Obstetrics and Gynecology, Faculty of Medicine, Tanta University, Tanta, Egypt.
*Corresponding Author: Nareman Elhamamy, Department of Obstetrics and Gynecology, Faculty of Medicine, Tanta University, Tanta, Egypt.
Citation: Elhamamy N, (2020) Evaluation of Fetal Mid-Thigh Soft Tissue Thickness and Femur Length for Estimation of Fetal Birth Weight. J Women Health Care Issues, 3(2); Doi:10.31579/2642-9756/023
Copyright: © 2020 Nareman Elhamamy, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 17 February 2020 | Accepted: 22 February 2021 | Published: 27 February 2020
Keywords: femur length; fetal birth weight
Accurate calculation of fetal weight relies on two equally important factors: the use of a formula with strong intrinsic properties, and the use of sonographic biometric parameters that are not susceptible to errors in measurement. From a statistical perspective, the inclusion of multiple variables in a model improves multicollinearity chances and decreases each measurement's internal error.
Precisely predicting estimated fetal weight during childbirth may have a significant impact on successful obstetric management, especially in the case of suspected macrosomia or low birth weight. Macrosomic fetuses can cause maternal and neonatal complications during childbirth, and low-born fetuses are at increased risk for perinatal morbidity and mortality.
The main aim of the study was to assess the accuracy of measurement of mid-thigh soft tissue thickness and femur length, in estimation of expected fetal birth weight
The study was conducted during the period January 2017 to August 2019, at Tanta University hospitals, Obstetrics & Gynecology department. 65 pregnant ladies at term (between 37-40weeks) were included in the study.
Results: Mean difference between fetal weight by Hadlock formulae and actual fetal weight is -10.88g; percent difference is (0.32%). The difference statistically insignificant p>0.05.
Mean difference between fetal weight by Scioscia’s formulae and Actual fetal weight is 2.83; the percent difference is (0.08%). The difference statistically insignificant p>0.05.
Good agreement between Hadlock formulae and Actual Fetal Weight Kappa value (0.73).Also shows moderate agreement between Scioscia’s formulae and Actual Fetal Weight Kappa value (0.52). area under curve Hadlock formulae (0.79), Scioscia’s formulae (0.78) for detecting fetal weight ≥3500gm among pregnant women at 39-40 weeks of gestation.
Conclusion: The mid-thigh soft tissue thickness and femur length can be used in estimation of expected fetal birth weight like as other sonographic parameters. The validity of Scioscia's formulae is not better than Hadlock formulae in detection of fetal weight less than 3500 gm. The validity of both formulae Scioscia's and Hadlock in detection of fetal weight more than 3500 gm. Reduced and cannot be dependable in extremes of weight.
Predicting the estimated fetal weight (EFW) during labor has a significant impact on adequate obstetric management, especially in cases of alleged macrosomia or low birth weight. During childbirth, macrosomic fetuses can cause maternal and neonatal complications and fetuses with low birth weight are at increased risk of perinatal morbidity and mortality [1].
In clinical practice, the EFW developed in the third trimester, typically around 30 weeks gestation, is widely used to predict the EFW on term, provided the fetus has a steady growth, but in all cases, it is not the truth [2].
Several studies have shown that fetal weight estimation in the third trimester does not enable us to determine the correct proportions of neither the small fetus nor the large fetuses, thereby raising the need to assess fetal weight closer to birth [3]. There are many calculations available to determine fetal weight based on standard fetal ultrasound measurements and the most precise are circumferential parameters such as head and abdominal circumference. Sadly, these parameters are more susceptible to intra-and inter-observer variability, particularly when these measurements are technically more difficult to obtain [4].
Scioscia M, et al, (2008) published a study proposing a novel method for EFW using femur length (FL) and mid-thigh soft tissue thickness (MSTT) measurements, including adipose tissue plus lean mass. With this formula, the authors sought to avoid imprecise and time-consuming circumferential measurements, allowing it to be applied conveniently even during labor [5,6].
To assess the accuracy of measurement of mid-thigh soft tissue thickness and femur length, in estimation of expected fetal birth weight.
Patients and methods
This was a prospective cohort study conducted during the period January 2017 to August 2019, at Tanta University hospitals, Obstetrics & Gynecology department. The subjects of the study were 65 singleton pregnant women admitted by elective cesarean section or labor induction and vaginal delivery within 48 hours for expected delivery at term (between 37-40weeks).
Selection of Patient:
All cases participated in the study were submitted to the following:
-General examination: including vital signs, body mass index and lower limb edema.
-Local examination (Abdominal examination): to confirm cephalic presentation.
All measurements were performed in the fetal ultrasonic unit using a 5.0 MHz convex probe (General Electric Logic p5) & Voluson730 pro trans-abdominal ultrasound.
In a single occasion, each fetus had been examined. Gestational age had been determined from the last menstrual period and confirmed by ultrasound, it was given in exact weeks. The patient lied in flat position, and after good exposure, application of conducting gel, A rapid overview performed first to confirm positive fetal life , longitudinal lie and cephalic presentation then parameters like Bi-parietal diameter (BPD), Head circumference (Hc) Abdominal Circumference (AC), Femur length (FL) and Mid-thigh soft tissue thickness (MTSTT) were measured respectively.
Biparietal diameter (BPD):
The longitudinal axis of the head was first calculated by finding the echo of the midline obtained from the falx cerebri taking into account the head's attitude. Next, the scanning probe was rotated 90 degree and named to correct the longitudinal axis inclination. The inner brain structures were examined until the basal ganglia and thalami were seen from the side to the midline of the head segment. [7].
Head circumference (HC):
After the long axis of the fetus is found, the transducer is turned 90 degrees to create a cross-sectional image of the fetal trunk, maintaining the angle of 90 degrees until the lower spine and the iliac crest are formed, then the transducer is rotated until an entire femur is imaged. The length of the femur is calculated to distal metaphysis from the greater trochanter [7].
Abdominal Circumference (AC):
AC Using the ellipse method, was measured in the same way as the head circumference. The long axis of the fetal body and its inclination were determined by identifying the aorta's longitudinal axis. The transducer was then rotated to match the long axis via an angle of 90 degrees. The transducer was then transferred to the plane that included the umbilical venous complex portal and obtains the fetal stomach [7].
Femur Length (FL):
The transducer is turned 90 degrees after the long axis of the fetus is identified to create a cross-sectional image of the fetal trunk, retaining the angle of 90 degrees until the lower spine and the iliac crest are established, then the transducer is rotated until a complete femur is imaged. The length of the femur is determined from the larger trochanter to the distal metaphysis [7].
Mid-thigh soft tissue thickness:
The mid-thigh STT was measured linearly from the outer edge of the skin down to the outer edge of the femur shaft using the same framed image. This measurement was taken in the middle of the fetal leg, so that the upper and lower trochanters were turned upward to ensure the correct view of the lateral side of the femur [8].
The estimated fetal body weight was calculated twice as follow:
1-Using the Hadlock formula determined by the programmed computer software, using B: the mid-thigh STT was measured linearly from the outer edge of the skin to the outer edge of the femur shaft using the same framed image. This measurement was taken at the mid-third of the fetal leg, so that the upper and lower trochanters were turned upward to ensure correct view of the femur.
2-Using Scioscia's formula, which had been calculated manually using FL and MTSTT as follow:
EFW= −1687.47 + (54.1× FL) + (76.68 ×MT STT)
N.B: FL by millimeter, MTSTT by millimeter.
The actual birth weight (ABW) of the infant was measured immediately after delivery and after cutting of the umbilical cord and clamping it 5 centimeters from the fetal abdomen without any towels or clothes. All fetuses were measured using the same calibrated scale.
This prospective study was analyzed and evaluated by comparing the results of EFBW using the previously illustrated Scioscia's formula [using femur length (FL) and Mid-thigh soft tissue thickness (MTSTT)] and already established commonly used Hadlock's formula [using bi-parietal diameter (BPD),head circumference(HC) abdominal circumference (AC) and femur length (FL)] with actual birth weight.
All data for windows (SPSS Inc., Chicago, IL, USA) were collected, tabulated, and statistically analyzed using SPSS 20.0. Quantitative data were expressed as mean ± SD and (minimum-maximum) and qualitative data as absolute frequencies (number) & relative frequencies (percentage) were expressed. T-test was used to compare normally distributed classes. Comparison of Paired t test. P-value < 0>
Receiver Operating Characteristic (ROC)
The Youden index was used to determine optimum cut-off. And measure the following: Sensitivity: likelihood that a test result will be positive when the disease is present (true positive rate, expressed as a percentage Specificity: probability that a test result will be negative if the disease is not present (true negative rate, expressed as a percentage Accuracy: equal to true positive + accurate).
Kappa coefficient
Here is one possible interpretation of Kappa coefficient measure agreement of two measures.
Poor agreement = Less than 0.20
Fair agreement = 0.20 to 0.40
Moderate agreement = 0.40 to 0.60
Good agreement = 0.60 to 0.80
Very good agreement = 0.80 to 1.00
Simple linear and multilinear regression:
Situations frequently occur in which we are interested in the dependency of a dependent variable on several independent variables
Formally, the model for multiple linear regressions, given n observations, is
Y = a + β1X1 + β2X2 + β3X3 +…….
Y= the variable that we are trying to predict
X = the variable that are using to predict
a= the intercept (Constant)
β = coefficient of x, represent the mean change in the dependent variable) for one unit of change in the predictor variable (independent), while holding other predictors in the model constant
t test =test of significant.
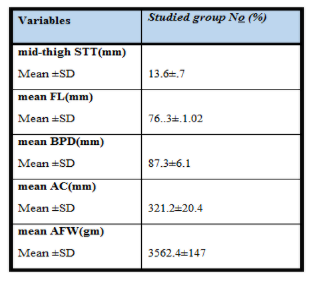
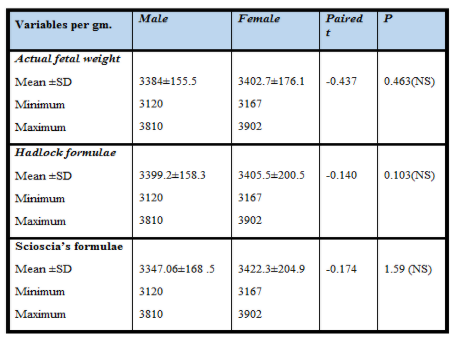
Table 1 shows the mean age of studied group is 26 year and minimum age is 19 year and maximum age is 34 year. Mean gestational age of studied group is 38 week and minimum Gestational age is 37 and maximum is 40 week. This table also define that prim gravid is 18.5% of studied group. As shown, there was no statistically significant difference between male and female regarding fetal weight by Hadlock formulae, Scioscia's formulae and Actual fetal weight per gm (Table 2,3).

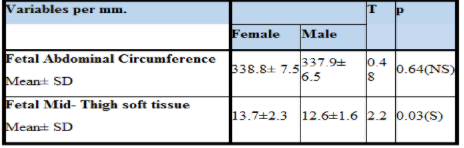
The mean of female Fetal Abdominal Circumference is 338.8 and male Fetal Abdominal Circumference is 337.9 the difference statistically insignificant p>0.05. Female Fetal mid- Thigh soft tissue is 13.7 and male Fetal mid- Thigh soft tissue is 12.6 the difference statistically significant p>0.05 (Table 3).
The Mean difference between fetal weight by Hadlock formulae and actual fetal weight is -10.88g; percent difference is (0.32%). The difference statistically insignificant p>0.05 (Table 4).
The Mean difference between fetal weight by Scioscia’s formulae and Actual fetal weight is 2.83, the percent difference is (0.08%). The difference statistically insignificant p>0.05 (Table 5).

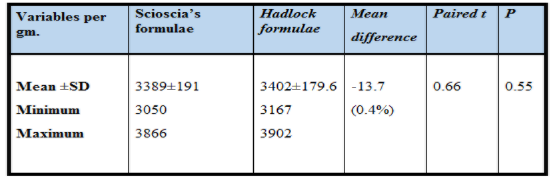
The Mean difference between fetal weight by Scioscia’s formulae and Hadlock formulae is -13.7 g, the percent difference is (0.4%). The difference statistically insignificant p>0.05 (Table 6).

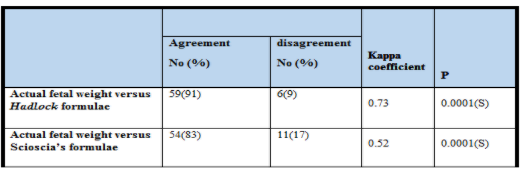
As showed in (Table 7) there is good agreement between Hadlock formulae and Actual Fetal Weight Kappa value (0.73).
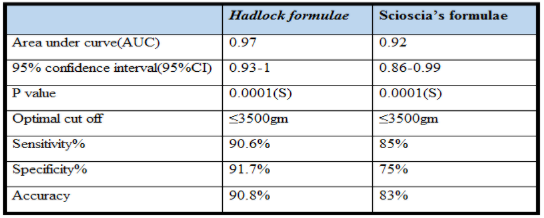
Also shows moderate agreement between Scioscia’s formulae and Actual Fetal Weight Kappa value (0.52). Hadlock formulae is more sensitive than Scioscia’s formulae for detection of fetal weight ≤ 3500gm with Sensitivity 90.6% for Hadlock formulae and 85% for Scioscia’s formulae and accuracy 90.8% for Hadlock formulae and 83% for Scioscia’s formulae which means that Hadlock is more dependable in detection of fetal weight less than 3500 gm (Table 8).
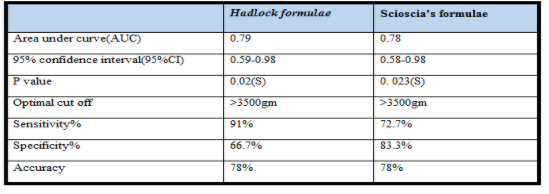
Hadlock formulae is more sensitive than Scioscia’s formulae for detection of fetal weight >3500gm among pregnant women at 39-40 weeks of gestation with Sensitivity 91% for Hadlock formulae and 72.7% for Scioscia’s formulae and accuracy 78% for both formulae which means that Scioscia’s formulae is not dependable in detection of fetal weight more than 3500 gm among pregnant women at 39-40 weeks of (Table 9,10) & (Figure 1,2).


Assessment of fetal weight, an important factor in assessing fetal survival, is necessary to detect any disruptions in fetal growth such as restriction of intrauterine development, and macrosomia. Both are at greater risk of mortality and perinatal morbidity. Thus, a reliable birth weight estimation will help to prevent some of these complications in the management of labor [9 ,10].
AC is widely accepted as the most valuable sonographic biometric parameter in fetal weight estimation; however, it is subjected to a significant intra-and inter-observer variability compared with linear measurements. Obtaining high quality images for measuring AC is not an easy job for some operators. Measurements taken from low quality images can lead to increased inter observer variability [11].
The present study has proposed that sonograghic measurements of fetal mid-thigh soft tissue thickness (MTSTT) in relation to femur length (FL) as a possible parameter for assessment of fetal birth weight.
The aim of our study was to evaluate the accuracy and usefulness of measuring femur length and mid-thigh soft tissue thickness in assessment of fetal birth weight by using Scioscia’s formula.
This is a prospective cohort study that was conducted during the period January 2017 to August 2019, at Tanta University hospitals, Obstetrics & Gynecology department and recruiting a total of 65 pregnant women who consented to participate in this study. All women considered for this study were at third trimester between 37-40 weeks gestation (confirmed by ultrasound and sure date of last menstrual period) and planned for delivery within 48 hours.
And this result nearly similar to the result in the study of Abuelghar et al., 2014 that assess Fetal mid-thigh soft-tissue thickness: a novel method for fetal weight estimation and found that the mean age of participants was 27.6 ± 5.5 years, the mean gestational age was 38.7 + 1.2 weeks. Among the study population, 67 women (22.3 %) were Para 1, 80 (26.7 %) were Para 2, 89 (29.7 %) were Para 3, 45 (15.0 %) were Para 4, 18 (6 %) were Para 5, and 1 (0.3 %) was Para 6 [6].
Agreement with our study, the study of Broere-Brown et al., 2016 found that HC and AC were larger in males than in females (0.30 SD [95% CI 0.26,0.34] and 0.09 SD [95% CI 0.05, 0.014], respectively). However, FL in males was smaller compared to female fetuses (0.21 SD [95% CI 0.17, 0.26]) [12].
This agrees with the study of Kurmanavicius et al., 2004 that found that among the five formulas for fetal weight estimation, the highest intraclass correlation coefficient was generated with both Hadlock formulas.
The best was Hadlock formula using 3 fetal biometry parameters (HC, AC and FL). The lowest intraclass correlation was found with Shepard formula. Accuracy of some of these formulas was shown to be more than previous ones with less percentage of error (4 ,5). The present study assessed fetal weight by Scioscia’s formulae and found that Mean difference between fetal weight by Scioscia’s formulae and Actual fetal weight is 2.83; the percent difference is (0.08%). The difference statistically insignificant p>0.05.
In accordance with our study, Kalantari et al., 2013 conducted prospective cohort study to find the impression of soft tissue thickness on birth weight and represent a new predictive formula. They included 114 pregnant women with normal singleton term (36-42w) pregnancies who delivered within 72 hours. They measured abdominal circumference, biparietal diameter, femur length and mid-thigh soft tissue thickness. The actual neonatal birth weight was also measured after birth. Linear regression model was used and R square and P-value was reported. They concluded that adding mid-thigh soft tissue thickness to the other variables in predictive models of fetal weight would provide a good estimation (r (2) =0.77) and in cases that measuring abdominal circumference is suboptimal mid-thigh soft tissue thickness may be a good replacement. Which support our finding in this study [13].
In contrast of concurrent study, Barros et al., 2016 Conducted a prospective study to determine the accuracy of fetal weight prediction by ultrasonography using the same method in our study that included longitudinal measurements of femur length (FL) and mid-thigh soft tissue thickness (STT). The study involved 145 singleton uncomplicated term pregnancies within 48 hours of delivery. Only pregnancies admitted to the labor ward with a cephalic fetus.
They found that there was a poor correlation between actual birth weight and the estimated fetal weight using a formula based on femur length and mid-thigh soft tissue thickness, both linear parameters. That differs from our study that we found that there was a good correlation between actual birth weight and expected fetal weight using a formula based on femur length and mid-thigh soft tissue thickness [14].
In the current study, we tested the different sonographic biometric parameters, choosing the mid-thigh STT and FL for the following reasons: compared to the circumferences, linear parameters are more reproducible and can be easily measured by healthcare providers with little expertise throughout ultrasonography (Scioscia et al., 2008), both are easily obtained from the FL measurers [15].
While in the study that was prospective observational study to with term singleton pregnancy along with other standard biometric parameters, i.e. BPD, HC, AC and FL, and MTSTT. The predicted birth weight was compared with actual neonatal birth weight soon after delivery and regression coefficients (R2) were determined for each of prediction models for comparing the accuracies. They found that addition of mid Find out how the inclusion of mid-thigh soft tissue thickness (MTSTT) in fetal weight measurement formulas historically focused on biparietal diameter (BPD), head circumference (HC), abdominal circumference (AC), and femur length (FL) increases the estimate of birth weight (BW). MTSTT has been tested in 100 women within 1 week of delivery -thigh soft tissue thickness (MTSTT) to other biometric variables in models of fetal weight estimation improves neonatal birth weight prediction. This sup ports our finding in this study [16].
Another study that emphasizes our result is that conducted by Abdalla N. et al., 2015 to assess Correlation between ultrasonographic soft-tissue thickness measurement of the fetal thigh (FTSTT) and selected anthropometric fetal and maternal parameters (17).
A total of 140 women with a single-term pregnancy were included in the report. Maternal and fetal anthropometric measurements have been analyzed. Hadlock formula was used to estimate fetal weight using head circumference (HC), abdomen. FTSTT was measured using the method of Scioscia M. et al.,2008 which used also in our study. Then, statistical analysis of the correlation between FTSTT and maternal anthropometric and fetal ultrasonographic parameters was performed. [5]
They concluded that FTSTT measurement may be helpful in estimating fetal weight, but it is not useful in the diagnosis of fetal macrosomia. Which support our finding in this study. Among ultrasonographically calculated fetal weight and BPD, HC, AC, FL and FTSTT, as well as between FTSTT and neonatal birth weight and duration, and maternal pregnancy and weight of pre-delivery (5). We concluded that FTSTT calculation may be useful in fetal weight estimation, but it is not useful in fetal macrosomy diagnosis.
Also, in agreement with our study, Scioscia M. et al., 2014 In 2014, a retrospective study was conducted to determine the accuracy of birthweight sonographic estimation in suspected macrosomic fetuses. This research assessed their equation performance based on linear soft tissue measurement above the fetal femur's external side. Sixty-two fetal patients were registered with alleged macrosomia Sonographic measurements were taken within 48 h that means a lower internal error in the prediction. This study supports the potential of this new approach for the estimation of birth weight in large fetuses based on sonographic linear measurements only [8].
From a purely statistical point of view, the presence of different variables in a formula increases the risk of multicollinearity and enhances the internal error of each measurement. Clinically, the proposed formula can be of practical use in situations in which head measurements cannot be taken properly due to fetal head engagement.
On the other hand, we excluded all breech presentations from this study, in which the fetal hip can be down into the pelvis, causing the thigh profile to be distorted. These events, however, only represent a small percentage of all deliveries. In addition, linear measurements are easier to obstetricians / midwives with little sonographic training and linear mea compared to circumferences [18]. Fetal weight testing is a critical and common aspect of antenatal care, not only in labor and delivery management, but often during high-risk pregnancy management and growth monitoring.
Restriction of intrauterine growth, or both. The potential complications associated with vaginal delivery include shoulder dystocia, brachial plexus injury, bone injury, and intrapartum asphyxia for excessively large fetuses, whereas maternal risks include birth canal and pelvic floor injury, increased vaginal and caesarean delivery rates, and postpartum hemorrhage. Although deletion of outlier data is a controversial practice in statistics, outlier values play an important role in mathematics. A formula derivation is based on a mathematical approach to finding the best fitting curve for a given set of points, so data quality control was carried out using Grubb's method. Extreme outliers were discarded. Multiple linear regression analysis was used to derive the birth weight prediction equation, with actual birth weight as the dependent variable [19]
Our analysis emphasizes the application of STT to other ultrasonic parameters to boost fetal weight prediction models and recommends more research on the subject of replacing AC with STT. We hope this can be useful in clinical practice particularly when measuring AC is distorted.
By comparing the expected fetal weight by Scioscia's formulae and Actual fetal weight the results were comparable so we can depend on Scioscia's formulae in detection of fetal weight. The validity of Scioscia's formulae is not better than Hadlock formulae in detection of fetal weight less than 3500 gm.
The validity of both formulae Scioscia's and Hadlock in detection of fetal weight more than 3500 gm. Reduced and cannot be dependable in extremes of weight.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
